
Applications in Orthopedic Surgery

Advanced Placental Allografts When Patients are in Need
Orthopedic surgical procedures may need an advanced intervention which covers and protects the wound and thereby supports the healing process. MIMEDX offers an array of advanced placental allografts that may be used in a variety of surgical applications to provide valuable benefits in patient care.
Examples of AMNIOFIX® and AMNIOCORD® used as a protective barrier over the surgical repair or replacement:

Product Advantages: AMNIOEFFECT®, AMNIOFIX, and AMNIOCORD
- Provide a protective barrier on wounds and thereby support development of granulation tissue and the healing process
- Terminally sterilized for additional level of safety
- AMNIOFIX & AMNIOEFFECT: PURION® process preserves Extracellular Matrix (ECM) components, including 300+ regulatory proteins1,2
- AMNIOCORD: PURION process preserves ECM components, including 250+ regulatory proteins3
Clinical Use Examples:
- Rotator cuff repair
- Tendon repair
- Total knee, ankle, or shoulder replacement
Case Studies:
How Physicians Use Our Products
Case study 1
Rotator Cuff Repair4
Clinical History
A 52-year-old male smoker with a right shoulder injury due to a minor fall onto his outstretched hand approximately one month prior to presentation. He reported immediate pain and popping in his right shoulder which he managed with over-the-counter medications. The pain had progressed to a level of 6 out of 10, which made it difficult to perform work activities and to sleep.
Physical exam: Active forward flexion of the right shoulder was 150 degrees. Empty can test was positive. Impingement signs were positive. There was tenderness over the bicipital groove and acromioclavicular joint, and he had pain with cross-body adduction. The patient underwent a steroid injection at his initial visit, and a course of physical therapy was ordered. Approximately two weeks after his steroid injection, the patient reported that the injection helped for a few days, but he continued to have pain and difficulty sleeping. An MRI demonstrated a focal full-thickness supraspinatus tear, long head of the biceps tendinopathy, osteoarthritis of the acromioclavicular joint, and a glenoid labrum tear.
Surgical Intervention
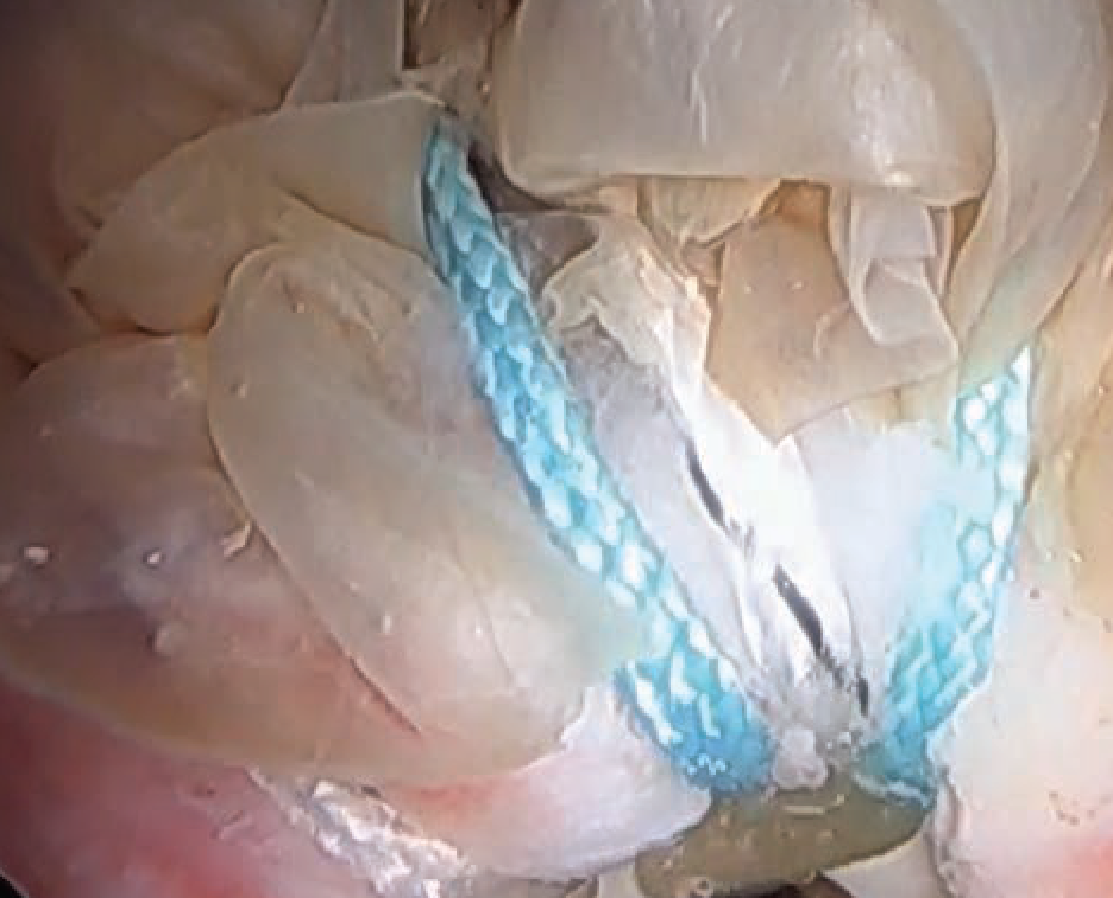
The patient underwent a right shoulder arthroscopy with rotator cuff repair and an application of AMNIOFIX placental allograft onlay over the repair.
Follow-Up
At the three month follow-up visit, function was excellent, and he returned to full work capacity, including overhead lifting and turning activities. Upon further follow up, the patient reported that his shoulder was doing well, and he declined a post-op MRI.
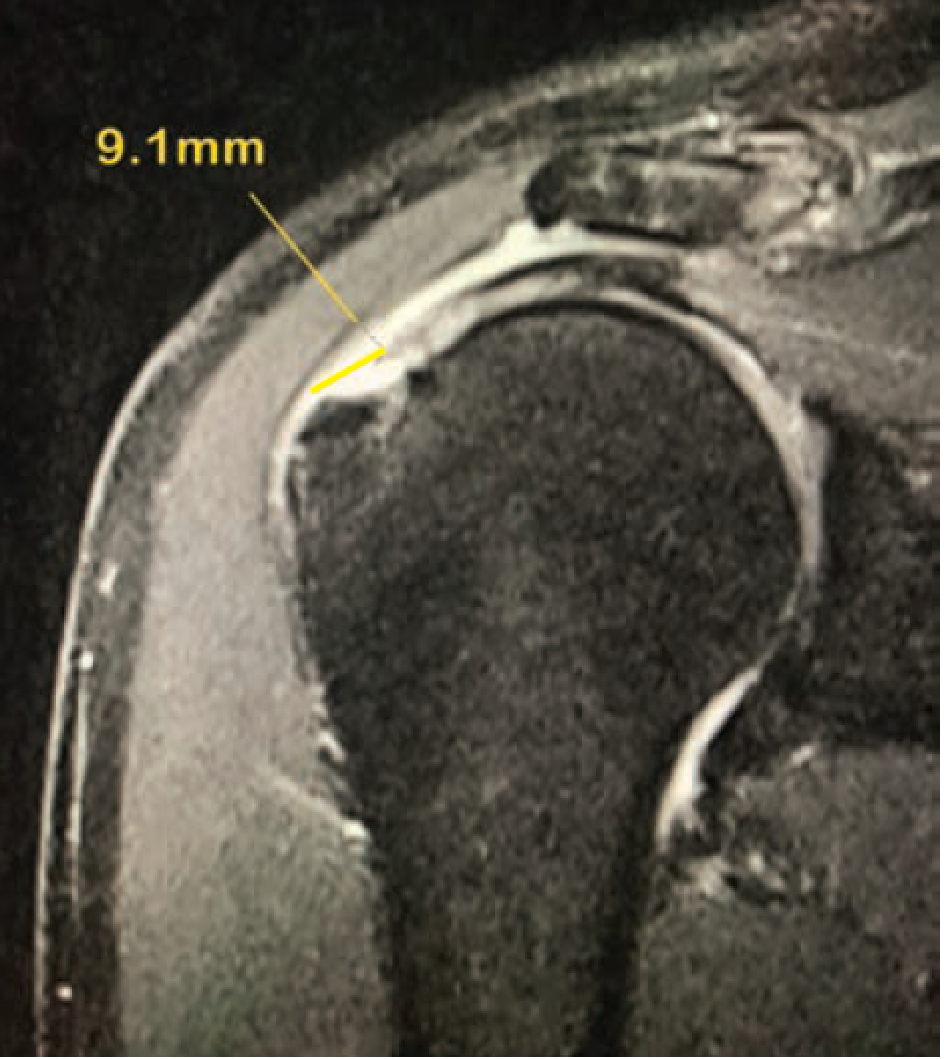 Pre-MRI: A focal full-thickness supraspinatus tear, long head biceps tendinopathy, osteoarthritis of the acromioclavicular joint, and a glenoid labrum tear Pre-MRI: A focal full-thickness supraspinatus tear, long head biceps tendinopathy, osteoarthritis of the acromioclavicular joint, and a glenoid labrum tear |
AMNIOFIX allograft secured to the repair site. |
Case study 2
Total Ankle Replacement5
Clinical History
A 65-year-old male presented with long-standing tenderness, swelling and stiffness in his right ankle. He was diagnosed with ankle arthritis. He failed conservative treatment including changing shoes, taking arthritis medications, cortisone injections, custom orthotics, and physical therapy. X-rays showed arthritis, and the patient was scheduled for a total ankle replacement.
Challenge
The extensor tendons, specifically the extensor halluces longus tendon, frequently become “stuck” in scar tissue with ankle arthritis, resulting in a stiff and painful ankle. Additionally, there is very little soft tissue between the ankle joint and the skin, posing increased risk for wound complications.
Surgical Intervention
The patient underwent a total ankle replacement. A standard, layered closure was done: deep capsule followed by tendon sheaths, subcutaneous tissue, then skin. AMNIOCORD was cut and applied around the extensor tendons to provide a protective barrier and thereby supported the healing process. The soft tissue and skin were closed over the AMNIOCORD, securing it in position.
Follow-Up
The patient was placed in a splint postoperatively and encouraged to ice and elevate the foot during the 1st postoperative week. Early range of motion exercises were started once the incision closed. He was able to return to his normal activities, including wearing normal shoes, three months after the procedure.
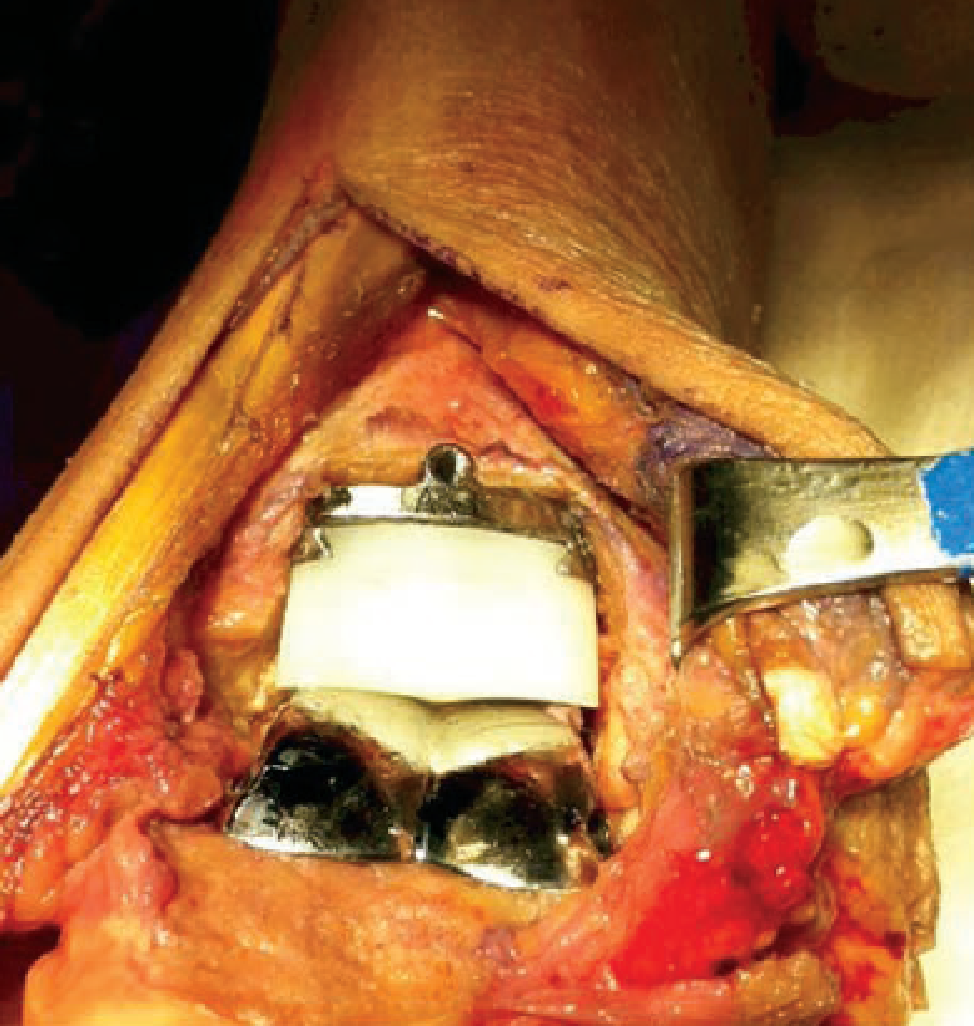
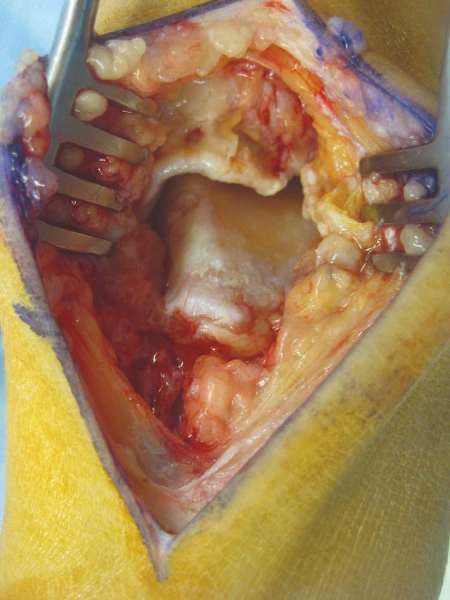
Total ankle replacement |

AMNIOCORD applied to extensor tendons / under skin closure |

Closed incision |
Case study 3
Repair of Ruptured Achilles Tendon6
Clinical History
A 45-year-old male suffered an Achilles tendon rupture while playing basketball. The patient had no previous history of injury to the affected ankle. Upon physical examination, the patient had swelling, bruising, and tenderness. There was a palpable defect present in the watershed region of the Achilles tendon and an absent Thompson test. Lateral X-ray of the ankle was normal. Ultrasound was performed and revealed a complete rupture of the Achilles tendon. Due to the patient’s activity level and the complete nature of the rupture, surgical repair was the selected course of action.
Surgical Intervention
A Flexor Hallucis Longus (FHL) fasciotomy was performed prior to the tendon repair to allow blood supply to the Achilles repair site and a tension-free peritenon closure. The Achilles was then repaired in standard fashion, and an epitenon suture was utilized circumferentially to reinforce the repair. A 3 cm x 5 cm AMNIOCORD umbilical cord allograft was placed directly over the repair site as a protective barrier and thereby supported the healing process. AMNIOCORD adhered well to the tendon and did not need to be sutured in place.
Follow-Up
The patient achieved closure uneventfully. At 6 weeks postop, physical therapy was initiated.
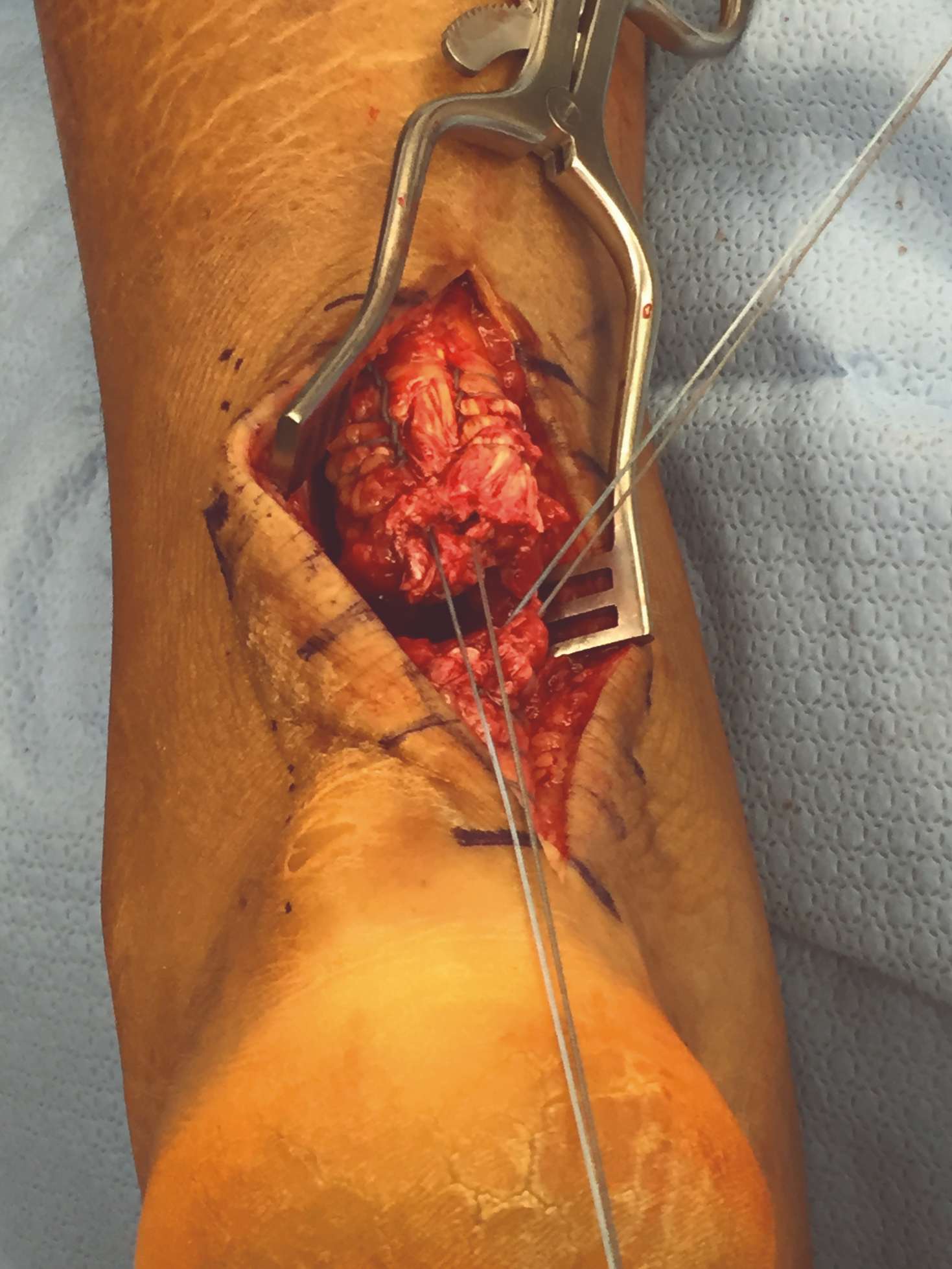
Placement of sutures to repair the ruptured Achilles tendon |
Achilles tendon rupture repaired |

AMNIOCORD placed as an onlay directly over the repair site |
Tips for Minimally Invasive Surgical (MIS) Procedures
- Cut allograft to desired size, if needed, prior to introduction into the port
- A minimum 8 mm port is recommended
- Assure an optimal field of view by suction/aspiration/evacuation of the relevant surgical field. This will optimize exposure and prevent accidental poor positioning or accidental removal of the allograft
- Surgical equipment and surgical site should be dry and clean of debris (pass gauze in and out of cannula)
- Ensure allograft is not hydrated / wet prior to introduction
- Use an atraumatic grasper to introduce the allograft sheet through the assistant port
Smaller Sheet Method

1. For a smaller sheet (e.g., 2 cm x 6 cm), grasp corner of allograft.

2. Wrap allograft around atraumatic grasper.

3. Hold the end of allograft in place while slowly and gently inserting it through cannula.

4. Release allograft from grasper and apply it to treatment area.
Resources
Surgical Product Portfolio: Advanced Placental Allografts
MIMEDX offers a portfolio of advanced placental allografts in the surgical setting.
- AMNIOFIX
- AMNIOCORD
- AMNIOEFFECT
- AMNIOBURN®
- AXIOFILL®
References
- Moreno S, Massee M, Campbell S, Bara H, Koob TJ, Harper JR. PURION® processed human amnion chorion membrane allografts retain material and biological properties supportive of soft tissue repair. J Biomater Appl. 2024;39(1):24-39.
- MIMEDX Internal Report. MM-RD-00086, Proteome Characterization of PURION Processed Dehydrated Human Amnion Chorion Membrane (dHACM) and PURION PLUS Processed Dehydrated Human Umbilical Cord (dHUC) Allografts.
- Bullard JD, Lei J, Lim JJ, Massee M, Fallon AM, Koob TJ. Evaluation of dehydrated human umbilical cord biological properties for wound care and soft tissue healing. J Biomed Mater Res B Appl Biomater. 2019;107(4):1035-1046.
- Brett Cascio, MD, Orthopedic Surgery and Sports Medicine, Lake Charles, LA.
- Daniel J. Cuttica, DO, Orthopedic Surgery, Falls Church, VA.
- Steven K. Neufeld, MD, Orthopedic Surgery, Falls Church, VA.
The case information presented reflects the clinical experience of the healthcare providers and is for educational purposes only. It is not meant to direct clinical decision-making. This presentation may include discussion of MIMEDX product use outside the product’s intended use. Please refer to the Instructions for Use for complete information, including tissue use.